|
Summary
A pelvic tumour, described as an ovarian cyst on preoperative ultrasound
examination, proved to be of small intestinal origin during the
exploration. Histologically, the resected tumor was diagnosed as
epithelioid leiomyoma. Nine years later a recurrent pelvic tumour was
found, suspected to be a malignant ovarian neoplasm. Exploration
revealed a large tumour of the ileum and several smaller tumors
dispersed in the pelvis.
Since at the time of the original diagnosis, GIST was a new entity,
little was known about the exact biological behavior and characteristic
histological signs of malignancy of this neoplasm. Our case demonstrates
that the epithelioid character of the tumor cells and the central
necrosis are, indeed, important features in the prediction of malignant
behavior, nevertheless, the absence of mitoses, absence of invasion of
the mucous and absence of increased cellularity in our case permitted
nine year disease-free survival. From the point of view of the
gynecologist, it is important to realize that not all pelvic tumors are
of reproductive system origin. This fact underlines the necessity of an
accurate preoperative diagnosis.
Key words: GIST, under-diagnosis of malignancy, pelvic tumor
Case report: 56-year-old thin female patient, admitted in November 1991,
diagnosed with ovarian cyst on ultrasound. She had no symptoms of
gynecological origin. In 1989, rectal bleeding of unknown etiology
occurred. Pre-admission clinical examination revealed a pelvic lump, the
size of a fist, with an uneven surface, partly firm and partly cystic.
Pelvic ultrasound examination revealed a partly solid and partly cystic
lesion, 9 cm in diameter, dislocating to the left the normal size
uterus. Result of cervical screening smear: P2. No pathological
abnormality was observed in laboratory tests. During the gynecological
explorative laparotomy, embedded in filamentous and lamellar adhesions,
a fist-size tumor was found adherent to the frontal surface of the
uterus, covered by a small intestine loop. With the adhesions cut
through, it became evident that the tumor originated in the small
intestinal wall. The reproductive organs were intact. An abdominal
surgeon was called in, who removed the affected section of the small
intestine and restored the continuity of the intestine with end-to-end
anastomosis. Following post-operative recovery, the patient was released
nine days after the operation, with a histopathological diagnosis of
epitheloid leiomyoma without evidence of malignancy. (Figure 1).
Nine years later, in October 2000, the patient contacted the clinic with
complaints of loss of appetite and weight. Abdominal ultrasound
examination revealed polycystic liver. This was assumed to be related to
the patient’s complaints of abdominal pain, to which partial resection
of the liver was considered as a possible treatment. Clinical
examination revealed a palpable pelvic tumor, and a subsequent
ultrasound examination revealed a 61 x 38 mm partly cystic and partly
solid lesion, the removal of which seemed more urgent. Laboratory tests
showed a slight anemia. There was no contraindication of the laparotomy.
The above examinations, again, led us to suspect a malignant ovarian
neoplasm. In order to establish whether the tumor had invaded the
surrounding structures, the following examinations were carried out: 1)
irrigoscopy - free passage of the colon up to the coecum, the volume and
haustration were normal, the retro rectal space was free, no organic
abnormality was seen; 2) cystoscopy - free passage of the uretra, normal
bladder mucous, normal urethra orifices, normal function; 3) MRI
revealed a 60 x 40 mm tumor on the left of the pelvis, with a moderate
signal intensity in Tl and high in T2; 4) Tumour marker CA 125: 26 lU/ml.
Because of the patient’s clinical history, an experienced surgeon was
requested to consult and then to participate in the operation. During
the laparotomy, a small intestinal loop adhering to the scar of the
first median laparotomy was injured and sutured. Cutting further
adhesions a fist-size small intestinal tumor was found. Several 1 cm to
3 cm metastasis tumors were found on the parietal peritoneum and the
serosal surface of the intestines. A few of these tumors were removed
for histopathological examination. During the mobilization of the
primary tumor adhering to the bladder, the vertex was injured and
subsequently treated with a two-layer suture. The tumor was removed with
a 15 cm section of the ileum. The continuity of the small intestine was
restored with an end-to-end anastomosis. The removal of extensive
metastases was unfeasible. Due to the adhesions only a partial
exploration of the liver was possible: on the lower surface of both
lobes, several 5 cm to 10 cm cysts were observed. Following irrigation
of the abdominal cavity with normal saline solution, the abdominal wall
was closed with one-layer suture.
In the post-operative period the patient was treated with antibiotics (Zinnat
+ Klion, then Dalacin) and recovered without complication. Her bowel
function returned to normal and had her bowels opened on the fourth
post-operative day. On the 10th post-operative day sutures and the
bladder catheter were removed. Histopathology showed malignant
gastrointestinal stoma tumor in each resected tissue. Probably the
nodules removed from the peritoneum and the omentum were metastatic
tumours of the ileal tumour rather than synchronous lesions. (Figure 2).
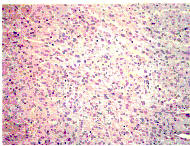
Figure 1.
The first tumour built up from elongated, plump cells
with eosinophilic cytoplasm.
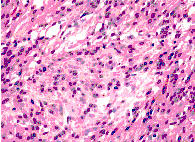
Figure 2.
More pleiomorphism, mitotic figures characterise the recurrent tumour
nine years later.
C-kit immunohistochemical reaction was
performed retrospectively on the primary and the recurrent tumour. The
primary tumour showed slight diffuse positivity. In the recurrent tumour,
the cells focally showed more pronounced positive reaction. Oncological/chemotherapeutic
treatment was decided.
Discussion
Mesenchymal tumours of the small intestine are rare, making up 20% to
25% of all tumours. They cause stenosis or obstruction or haemorrhage.
In cases of pelvic tumours, it may be difficult to distinguish them from
tumours of gynaecological origin, primarily of ovarian tumours. Since
the latter are significantly more common, such small intestinal tumours
may be discovered during gynaecological exploration.
Gastrointestinal stoma tumours were described in the late 1980s. This
type of tumours includes c-kit positive, mesenchymal tumours
differentiated in various directions l. It is difficult to predict the
biological behaviour of these neoplasms and the morphological
characteristics defining dignity were not described until some years ago
2. In retrospect, only the size, central necrosis and, histologically,
the epithelioid appearance of the tumour removed in the first operation
could have indicated the high probability of recurrence and metastases.
Further histological signs of potentially malignant behaviour, namely,
high cellularity, a high mitotic rate and mucosal invasion were not
present in the first tumour. The recognition of the recurrence of the
disease was made difficult by the presence of an extremely enlarged,
polycystic liver, in as much as the symptoms it caused partly diverted
attention from pelvic symptoms. Results of imaging suggested that the
liver disease was more severe than the space occupying process in the
pelvis.
We considered it important to describe the patient’s history for the
following reasons:
1) Searching literature data, only one similar case has been reported so
far 3.
2) Even the latest imaging techniques do not always reveal
preoperatively the exact origin of a tumour believed to be of ovarian
origin.
3) The rapid accumulation of data and increase of experience in the
field of pathology may lead to the re-assessment of entities described
earlier. Consequently, the follow-up of patients with rare types of
tumours is especially important.
4) In cases of pelvic tumours of uncertain origin it is advisable to
have a surgeon and/or urologist standing by for consultation.
5) In such cases an appropriate pre-operative prophylactic bowel
preparation is necessary. |
|
Literature:
1. Miettinen M, Kopczynski J, Makhlouf HR,
Sarlomo-Rikala M, Gyorffy H, Burke A, Sobin LH, Lasota J.
Gastrointestinal stromal tumors, intramural leiomyomas, and
leiomyosarcomas in the duodenum: a clinicopathologic,
immunohistochemical, and molecular genetic study of 167 cases. Am J Surg
Pathol 27:625-641, 2003.
2. Miettinen M, El-Rifai W, Sobin HL, Lasota J. Evaluation of malignancy
and prognosis of gastrointestinal stromal tumors: a review. Hum Pathol
33:478-483, 2002.
3. Long CY, Lee YM, tsai KB, Su JH, Hsu SC. Primary jejunal
leiomyosarcoma mimicking a gynecologic tumor. Gynecol Obstet Invest
54:180-182, 2002.
|